





PANTHER LIFE SCIENCES
Helena is an investor in Panther Life Sciences, a biotechnology company developing the microarray patch as a new infrastructure for vaccine and therapeutic delivery.
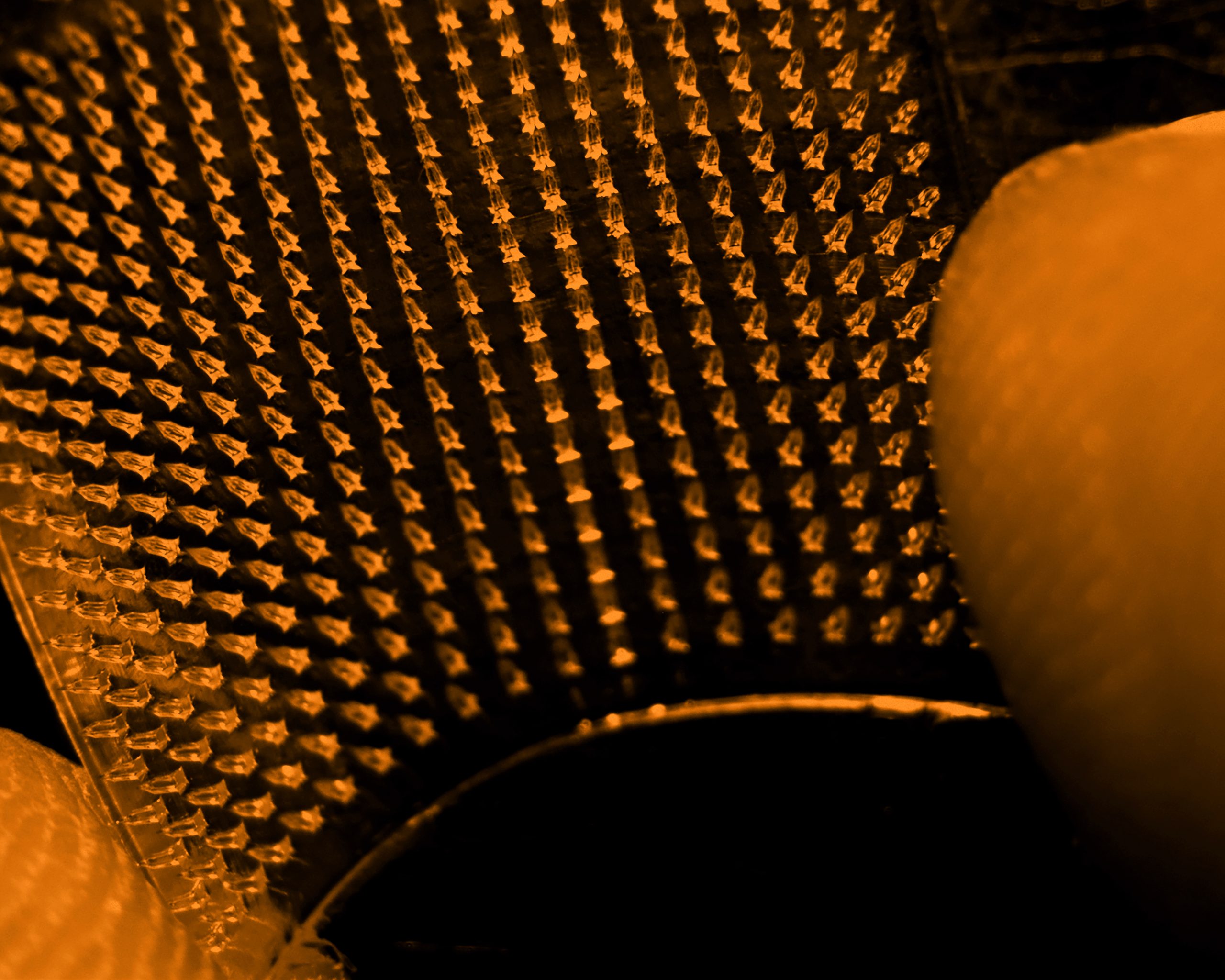
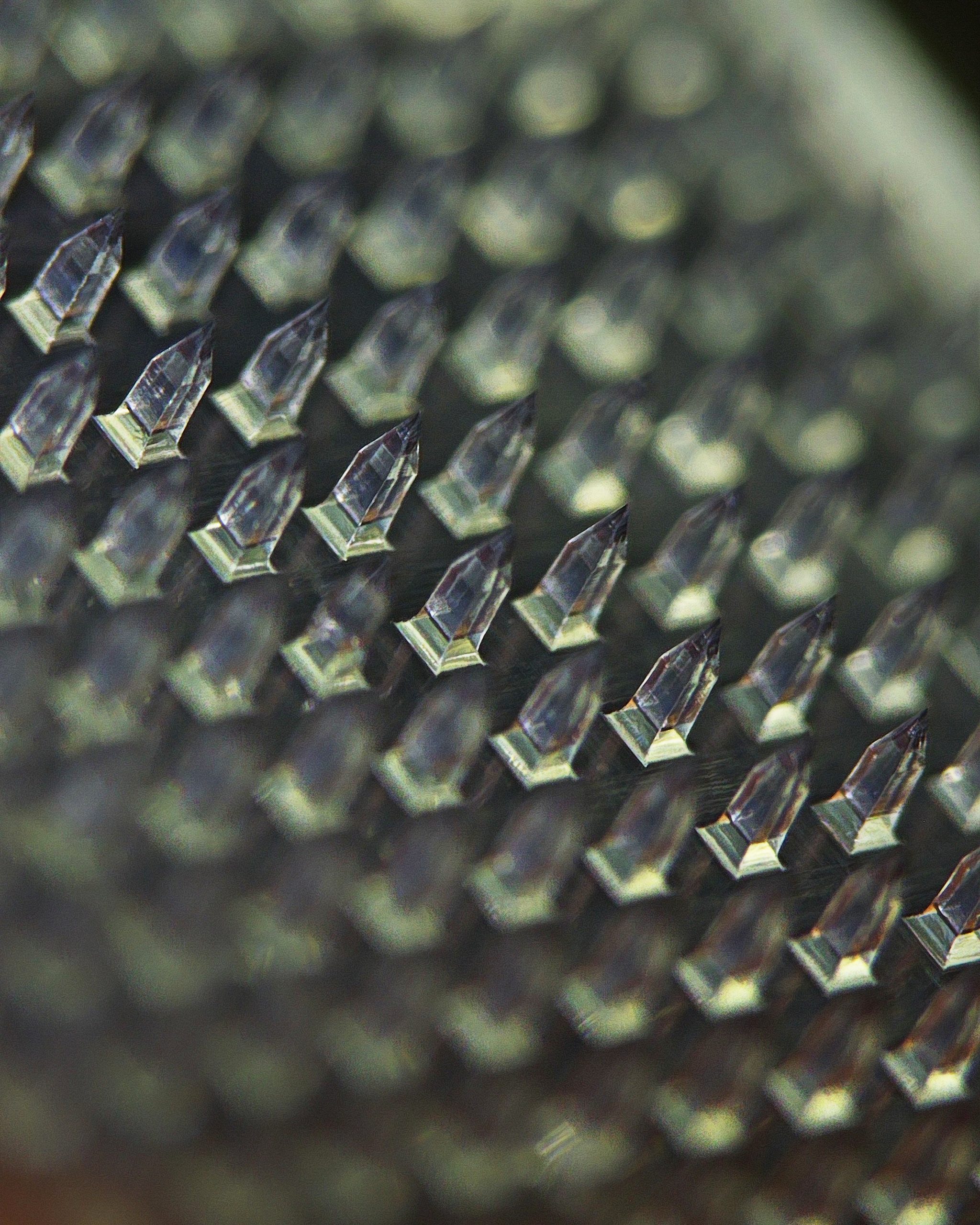
The patch is small, shelf-stable, and embedded with hundreds of dissolvable microneedles that release their payload directly into the immune-rich layers of the skin.

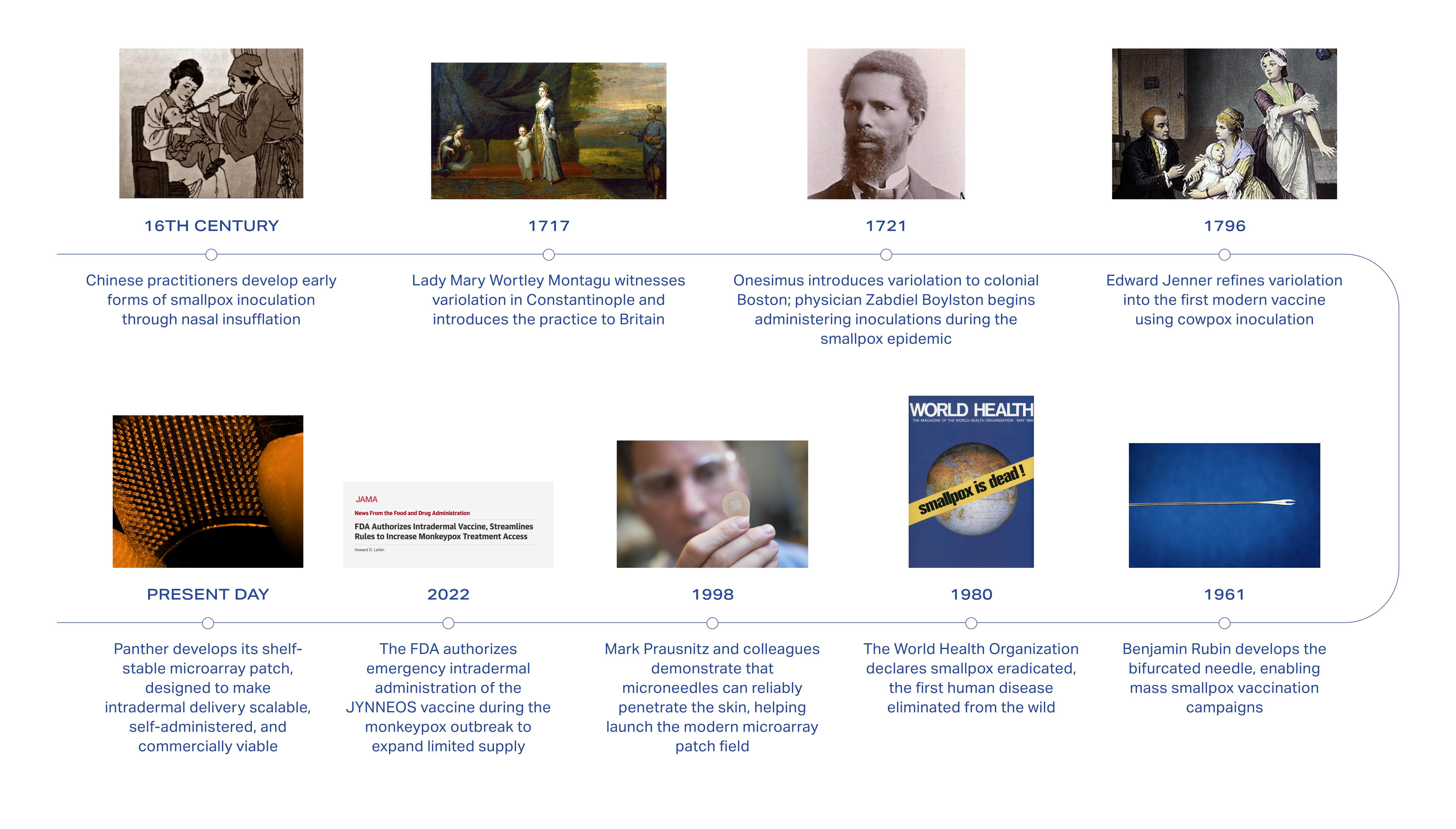
The underlying insight is centuries old. In the 18th century, women in Constantinople were variolating children against smallpox through small punctures in the skin. Edward Jenner refined the practice seventy-five years later, in a Gloucestershire village, and gave it the name that endures. When the World Health Organization eradicated smallpox in 1980, the only human disease ever erased from the wild, it did so with a bifurcated needle designed to deposit vaccine into the upper layers of the dermis. For as long as vaccination has existed, the skin has been its most productive target.
The intramuscular syringe that dominates modern medicine is a twentieth-century convenience. It displaced the older practice for reasons of manufacturing and training. Biology had little to do with it. And it came at a cost whose scale only the last five years have made visible: a global pharmaceutical system that, when a pandemic arrives, cannot deliver its own vaccines to most of the world.
As much as a quarter to half of all vaccines fail to reach a patient, depending on the metric. More than fourteen million infants worldwide received no routine vaccination at all last year, more than half of them in fragile and conflict-affected countries. The global pharmaceutical cold chain costs more than thirty billion dollars a year in logistics, wastage, and losses.
A shelf-stable patch that could replace the syringe has been a recurring dream of drug delivery research since the 1970s. A succession of well-funded companies has tried to build it: Theraject, Corium, Zosano, Vaxxas, Vaxess, Micron Biomedical. None has made it commercially real, because every attempt began at the top of the therapeutic pyramid, where regulatory review is longest, capital cycles are tightest, and no revenue arrives for a decade or more.
Panther, founded in Pittsburgh in September of 2023, is sequencing the problem differently. Its earliest products are a long-lasting hyaluronic acid patch for skin aging, targeted for market entry by the end of 2026, and a reformulated treatment for actinic keratosis, a precancerous skin condition that affects more than forty million Americans, targeted for around 2028.
The deeper pipeline, including infectious disease vaccines and tolerance induction for allergic and autoimmune conditions, sits years behind those launches, riding on the manufacturing line, the regulatory precedent, and the revenue the consumer and dermatology products will have already built. The science is anchored in a founding collaboration between Carnegie Mellon University and the University of Pittsburgh, and the manufacturing is housed at Pitt BioForge, the advanced biomanufacturing institute at the heart of Pittsburgh’s current biomedical reindustrialization.
A shelf-stable patch that can be mailed and self-applied removes, in a single motion, the four hidden constraints on which modern medicine currently runs: the cold chain, the clinician, the syringe, and the intramuscular dose. If the platform holds, the downstream implications reach pandemic preparedness, vaccine equity in low- and middle-income countries, the next generation of cancer immunotherapy, and the daily management of chronic disease.
Helena is supporting Panther because Panther is attempting to solve the part of this problem that has historically kept the field from becoming real. The science has been ready for some time. What the field has lacked is commercial sequencing, manufacturing scale, and regulatory legibility, and every previous attempt has run out of money trying to assemble those things.
The Infrastructure of Modern Medicine
In December of 2020, the first commercial doses of the Pfizer-BioNTech COVID-19 vaccine arrived in American cities inside what the company called thermal shippers.
Each was a white cardboard box the size of carry-on luggage, packed with twenty-three kilograms of dry ice and fitted with GPS sensors that fired an alarm if the internal temperature rose above minus sixty degrees Celsius. A single shipper held roughly five thousand doses. Once thawed and diluted with sterile saline, the vials had to be administered within six hours. Nurses raced clocks, and pharmacy managers chased no-shows by phone. In hospitals across the country, refrigerators designed for a different category of medicine were pressed into use. Hundreds of thousands of doses expired in syringes that had already been drawn.
It was one of the great logistical feats of the twenty-first century; it was also a portrait of how fragile the infrastructure of modern medicine still is.
A vaccine is a scientific object, whereas vaccination is a logistical event. Over the past hundred years, the first has been transformed beyond recognition, from inactivated whole-virus preparations through recombinant subunit vaccines to mRNA. The second, however, has barely changed since the postwar polio campaigns. The vials are still glass, the needles are still steel, and the freezers still need power.
This logistical feat traveled unevenly. By early 2022, high-income countries had administered roughly two hundred doses for every hundred people. Low-income countries had administered fewer than twenty. By that point, global mRNA production had begun to catch demand. The limit was the last fifty feet of delivery: the freezer at the health post, the clinic with electricity through the afternoon, the nurse who knew how to reconstitute an mRNA dose, the syringe, the sharps bin, the cold-box-equipped motorbike that would carry the next batch to the village. The pandemic revealed, in compressed and visible form, a problem that had been there the whole time.
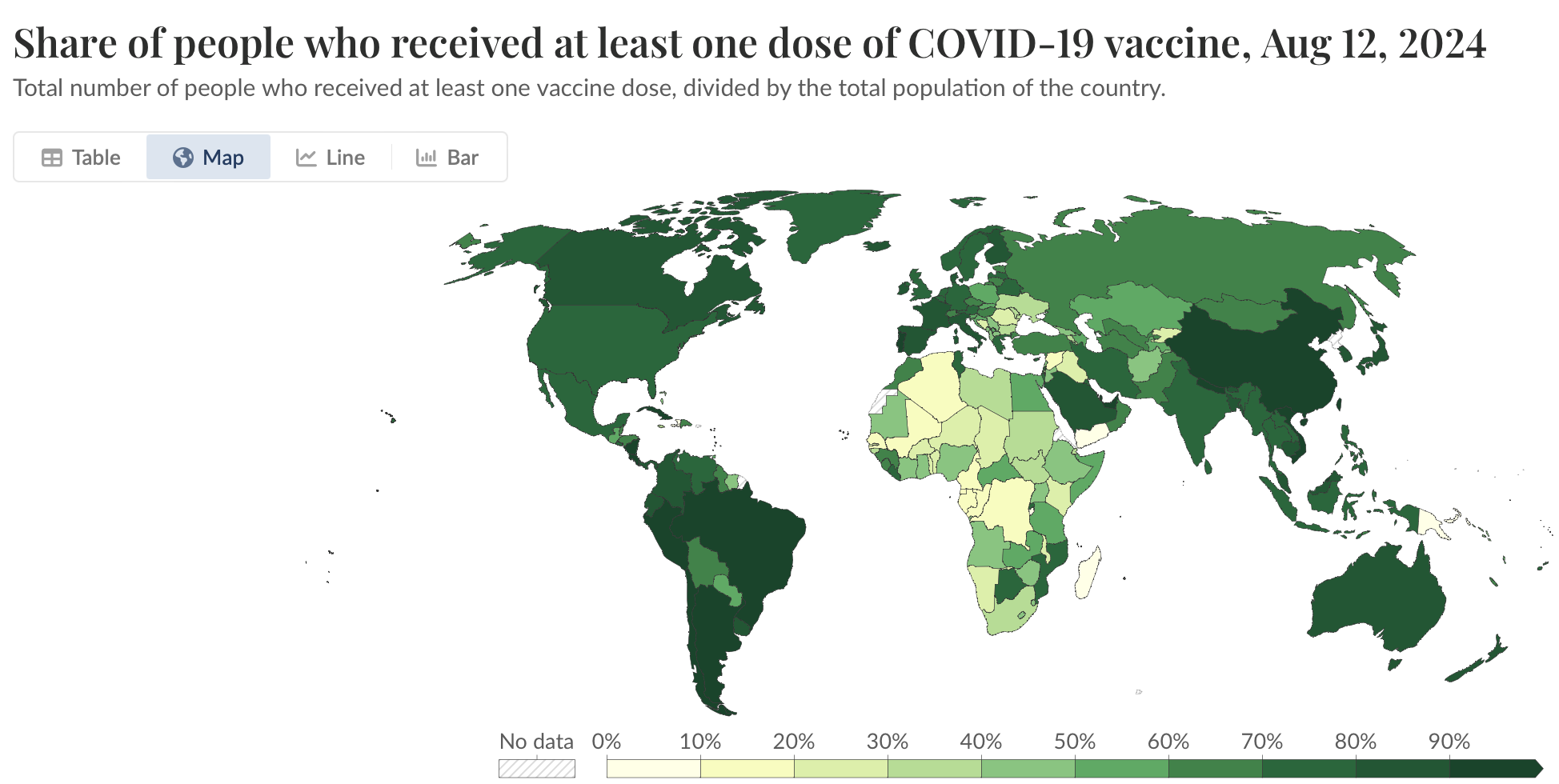
As much as a quarter to half of the world’s vaccines are degraded or spoiled by the time they reach a patient. This cold chain costs the U.S. healthcare system tens of billions of dollars a year in logistics, wastage, and losses. In low- and middle-income countries, the costs are less often calculated in dollars and more often in absence. More than fourteen million infants received no routine vaccination at all last year, whether that be for measles, diphtheria, tetanus, or polio.
Every one of those vaccines exists, and not one of them could reach those children. Even in countries with the freezers, the last fifty feet are porous. Around three hundred and eighty-five thousand sharps injuries occur in American hospitals every year. Needle phobia is now recognized as a measurable contributor to vaccine hesitancy; in the 2023–2024 influenza season, only thirty-six percent of American adults chose to be vaccinated. Half of patients prescribed chronic-disease medications fail to take them as directed. Every one of these failures has a clinic, a syringe, and a moment of discomfort at its center.
Then there is the dose itself. Almost every injectable vaccine in the world is delivered into muscle. Muscle is a convenient target: it is easy to find, easy to inject, well-vascularized. Muscle, however, is not an immune organ. The antibody response a muscle can mount is the result of antigen traveling from that depot outward to the lymph nodes, where the actual immune work happens. Because the tissue is comparatively inert, we use more antigen per dose to get the response we want, often an order of magnitude more than we would need if we were delivering somewhere better.
It is a strange historical accident that the default delivery site for the immunizations of the modern world is not an immune organ. The accident has cost us decades of supply, decades of coverage, and a pandemic’s worth of inequity. The question, which resurfaces in the scientific literature every generation and never quite finds a commercial answer, is what it would look like to aim somewhere else.
Why the Skin Has Been the Answer All Along
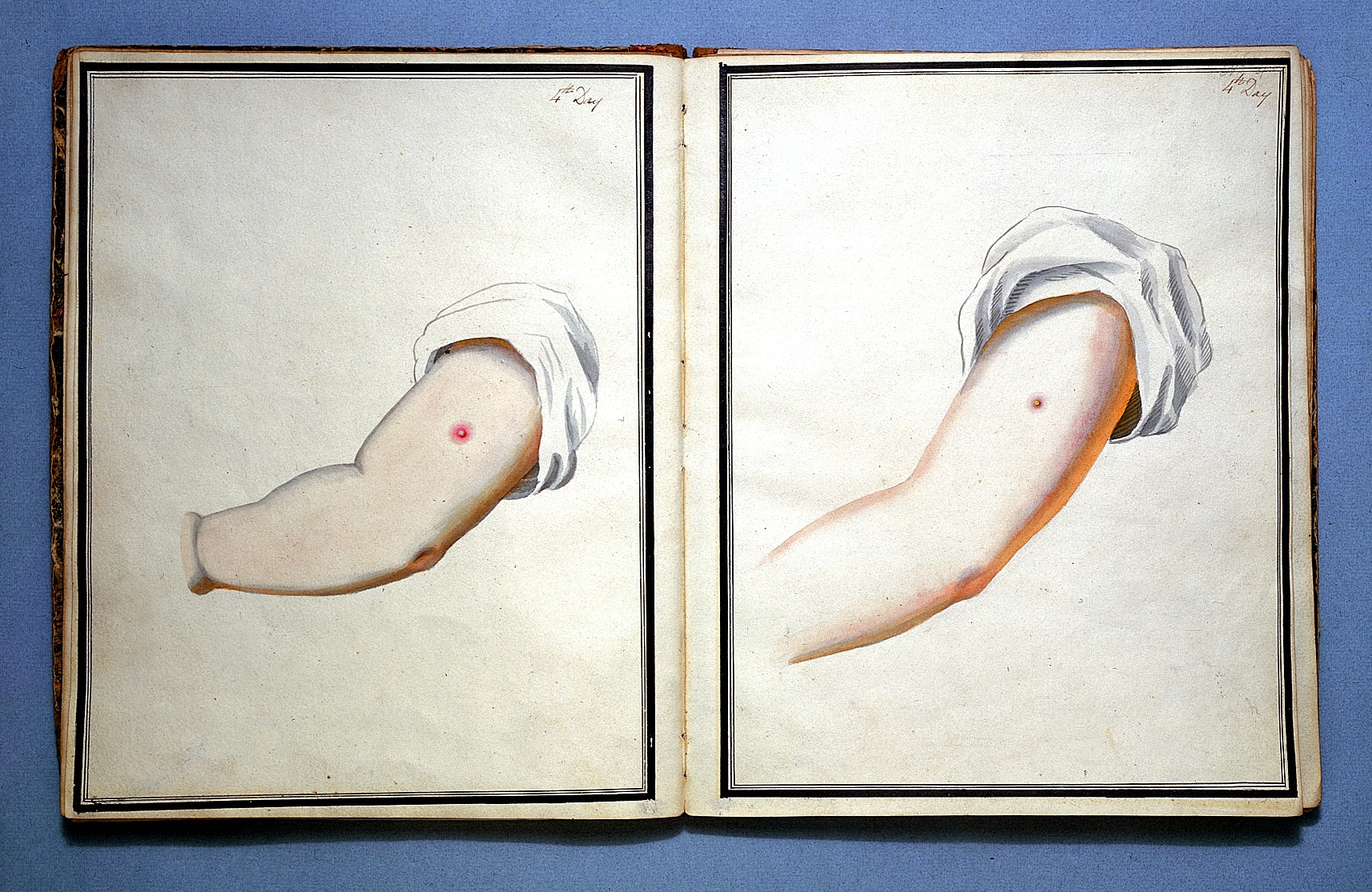
In the spring of 1717, Lady Mary Wortley Montagu, the wife of the newly-appointed British ambassador to the Ottoman Empire, watched Greek women in Constantinople perform a ritual that had been practiced across parts of Asia and Africa for centuries. One woman would open a nut-shell filled with pus from a smallpox lesion, dip in a needle, and prick the skin of a healthy child in four or five places, introducing a small amount of the virus under the epidermis. The child would develop a mild case of smallpox and, afterward, be immune for life.
Lady Mary, whose own face had been scarred by the disease and whose brother had died of it, had her nearly-five-year-old son variolated in Constantinople in March of 1718. Three years later, in April of 1721, in the middle of a London smallpox outbreak, she arranged for her three-year-old daughter to be variolated in front of the royal physicians. Her daughter survived. The Princess of Wales ordered trials on condemned prisoners and orphans. On the back of this success, variolation passed into English medicine, and then into the colonies.

In the same summer of 1721, on the other side of the Atlantic, Boston was in the middle of its own smallpox outbreak. An enslaved West African man named Onesimus had told his enslaver, the Puritan minister Cotton Mather, that in the country of his birth it had been common practice to rub smallpox matter into a small cut in the arm. Mather, with the reluctant help of a physician named Zabdiel Boylston, began conducting variolations during the epidemic. The results were striking. Of the roughly six thousand Bostonians who contracted smallpox naturally that year, fourteen percent died. Of the two hundred and forty-seven Boylston variolated, fewer than three percent did.
Seventy-five years later, in the English county of Gloucestershire, a country doctor named Edward Jenner refined the practice into vaccination. On May 14th, 1796, Jenner took a bit of material from a cowpox lesion on the hand of a milkmaid named Sarah Nelmes and pressed it, through a pair of small scratches, into the arm of an eight-year-old boy named James Phipps. Six weeks later, he exposed the boy to smallpox. Nothing happened. Jenner’s technique was intradermal. So was Montagu’s. So was Onesimus’s. So were the Chinese insufflations that predated both. The modern practice of vaccination began in the skin.
The same instinct guided the eradication campaign that finally ended smallpox forever. In 1961, a microbiologist at Wyeth Laboratories named Benjamin Rubin developed a small, inexpensive bifurcated needle that held a droplet of vaccine between its two prongs. In the field, vaccinators came to deliver each dose through fifteen rapid strokes into the upper layers of the skin. The bifurcated needle was the workhorse of the World Health Organization’s Smallpox Eradication Program, from its expansion in 1967 through the last naturally-occurring case in Somalia in 1977. When the WHO certified eradication in 1980, the only human disease ever erased from the wild, it was the skin that had done it.

The reason the skin works so well is architectural. The skin is the body’s outermost immune organ, built to distinguish self from non-self at the point of contact with the outside world. The epidermis, a sliver of tissue no thicker than a human hair, is seeded with Langerhans cells. These antigen-presenting sentinels were first described in 1868 by a twenty-one-year-old German medical student named Paul Langerhans, who was trying to prove that a particular class of cells in the skin were part of the nervous system, and instead, in the process, discovered part of the immune one. Beneath them, in the thicker dermis, sits a richer and more varied population of dendritic cells. The entire family was characterized in 1973 by an immunologist at Rockefeller University named Ralph Steinman, who was awarded the Nobel Prize for the work in 2011, three days after his death from pancreatic cancer. Alongside them live resident memory T cells, macrophages, mast cells, and a lymphatic network that drains directly into the regional lymph nodes. Square centimeter for square centimeter, no other accessible tissue in the human body is more primed to answer an antigen than the dermis.
For many vaccines and immune-active therapeutics, the skin is a more efficient delivery site than muscle. The intramuscular syringe came to dominate for reasons of standardization, training, and manufacturing rather than biological superiority.

Modern medicine has quietly rediscovered this older truth more than once. In the summer of 2022, the United States faced a severe shortage of the JYNNEOS smallpox vaccine in the middle of an MPox outbreak. The outbreak was spreading fastest through gay and bisexual communities in New York, Washington, San Francisco, and Atlanta. The Food and Drug Administration issued an emergency authorization for intradermal administration at one-fifth the standard subcutaneous dose. The clinical evidence, drawn from studies that had been on file since 2015 and from real-world data gathered through the summer, suggested that the smaller intradermal dose produced an immune response comparable to the full dose delivered below the skin. Overnight, a fixed supply became five times larger, and public health officials in the hardest-hit cities breathed a quiet sigh of relief. The announcement passed with little fanfare outside the community it served, but it was a federal admission that the ordinary way we deliver vaccines leaves a great deal of efficacy on the table.
The pattern is repeating with mRNA. Research groups in the Netherlands, Thailand, and the United States have shown, through 2021 and 2022, that one-fifth doses of mRNA COVID-19 vaccines administered intradermally produce antibody responses at least as strong as the standard intramuscular ones. For every COVID shot the world managed to manufacture during 2021, the same antigen stockpile could have produced several times as many intradermal equivalents. Those equivalents could have traveled in ordinary envelopes.
The only thing standing in the way has been the device.
The Commercial Graveyard of the Microneedle Patch
The idea of delivering drugs through arrays of tiny needles is decades old. In 1976, two scientists at the Alza Corporation named Martin Gerstel and Virgil Place filed a U.S. patent, 3,964,482, for “a device for delivering a drug through skin” using “a plurality of microprojections.” The patent was, as these things go, quiet. No product resulted. The concept drifted in the scientific literature for another two decades before it returned in earnest, this time in a corner of the Georgia Institute of Technology campus, in an unassuming laboratory run by a chemical engineer named Mark Prausnitz.
Prausnitz began working on microneedles in 1998, when the prevailing assumption among drug delivery researchers was that anything smaller than a standard hypodermic needle would not actually pierce the skin. He and his students proved the assumption wrong. Arrays of needles on the scale of hundreds of microns could penetrate the tough outer layer of dead skin, the stratum corneum, without reaching the pain-sensitive nerves of the dermis. You could inject a drug into the skin without the patient feeling the needle go in. A first wave of papers landed; a second followed, and the field reopened.
From that moment forward, the dream was unambiguous. A disposable patch the size of a coin, carrying a dose in the tips of its dissolving needles, could be applied in a minute of skin contact and then thrown away. It could be shipped without a freezer. It could be mailed. It could be applied by anyone, anywhere, without a clinician. Global vaccine distribution could be reimagined, and the developing-world coverage could catch up with the developed world’s. Pandemics could be answered with a supply chain that looked more like Amazon than UPS.
For nearly thirty years, a succession of companies set out to build that patch. Theraject, Nanopass, Zosano, Vaxxas, Vaxess, Micron Biomedical. Each had excellent scientists, and each had serious venture backing. Each believed, reasonably, that the next clinical readout would be lead to success. And yet, with rare exceptions, the pattern was the same. A company would close a large round, pick an ambitious therapeutic target (a migraine drug, a parathyroid hormone for osteoporosis, an influenza vaccine), and spend the next several years pushing it through trials. The manufacturing would cost more than projected; the regulatory path would stretch longer than hoped; the revenue horizon would keep receding. Then, investors would tire. The company would miss a clinical endpoint, or run out of cash, or watch its manufacturing partner back out. Finally, the dream would defer for another five years.
The clearest example is Zosano Pharma, a company founded in 2006 around a zolmitriptan microneedle patch for migraine. Zosano had good science and a real, working product. It relieved migraine within thirty minutes, faster than the best oral formulations available. But in October of 2020, the FDA issued a Complete Response Letter citing inconsistent drug exposures across the company’s clinical pharmacology studies, traceable to variability between manufacturing lots of the patches themselves. The agency wanted a repeat bioequivalence study and additional product quality data before it would consider the drug. Zosano spent the next year and a half preparing a resubmission, negotiating with the FDA, laying off staff, and burning through cash. In June of 2022, after sixteen years and more than a hundred million dollars in cumulative investment, the company filed for Chapter 11 bankruptcy in Delaware. Its intradermal delivery technology was sold off in the proceedings. The patch had worked in the body; however, it couldn’t be manufactured reliably enough to pass a combination-product review, and therefore it never reached a patient.

The skin’s behavior is well understood. Hundreds of peer-reviewed studies have shown that a well-designed microneedle array does, in a patient, what its designers hoped it would do. The barrier has been somewhere else, in a place biology cannot reach: in manufacturing, regulation, and capital, interlocked in a way that has turned out to be uniquely unforgiving for a first-of-its-kind combination product.
Manufacturing a microneedle array at clinical quality is a problem in materials science that the field consistently underestimated. The needles must be formed, loaded with a precise dose of drug, kept stable at room temperature for months, and delivered reliably to the same depth of skin in every patient. Early processes were artisanal: careful laboratory benchwork adapted for a hundred patches at a time. At Phase I scale, artisanal works; however, at commercial scale, where a single vaccine indication might require tens of millions of units a year, unit economics have historically collapsed. A patch that cost five dollars to produce when a dose of vaccine cost fifty cents was not a product.
Regulation compounded the problem. A microarray patch is a combination product, a drug and a device at once, and the FDA reviews each separately and together. Either pathway is long and expensive on its own. Stacked, they can demand a decade and hundreds of millions of dollars before a company ships its first commercial unit. For a pre-revenue biotech, that runway is hard to raise and harder to hold.

The science had been ready for a long time. What the field needed was a commercial strategy that could build the manufacturing, the regulatory precedent, the real-world data, and the supply chain without requiring a vaccine approval to pay the bills.
Panther's Inversion
The research community that would eventually produce Panther had been assembling in Pittsburgh for more than a decade before the company existed.
The University of Pittsburgh’s Department of Dermatology, under the leadership of its chair, Louis Falo, had been working on microneedle technology since the mid-2000s. Falo, an immunologist by training with a deep interest in skin-based vaccines, was particularly interested in the dermis as a site for cancer immunotherapy. By the 2010s, his laboratory had built, in collaboration with the University of Pittsburgh’s bioengineering department, a set of microneedle designs of unusual scientific depth. Emrullah Korkmaz, a young Pittsburgh bioengineer who had joined the department after his PhD, began developing manufacturing techniques for the arrays that would later become the basis of Panther’s platform. Across the street, at Carnegie Mellon, a group led by Gary Fedder at the university’s Institute for Complex Engineered Systems, and by Douglas Weber in mechanical engineering, was working on adjacent problems in microfabrication and in the neural engineering of implanted devices. Together, Pittsburgh and Carnegie Mellon had assembled, without much fanfare, one of the deepest microneedle research communities in the world.

The funding that kept the work going was primarily non-dilutive, and largely federal. The Department of Defense, the Walter Reed Army Institute of Research, the Uniformed Services University of the Health Sciences, DARPA, and the Wellcome Leap program, a global health-research organization funded by the Wellcome Trust and overseen in its first years by Ken Gabriel, all found in the Pittsburgh group a set of capabilities that matched their interests in rapid-response vaccines, biodefense countermeasures, and oncology immunotherapy. Over the decade, the research program drew more than seventy-five million dollars in support. Patents accumulated. Clinical programs reached Phase II, under partnership with academic medical centers. But it remained, in a meaningful sense, research. There was no company.
The missing piece was a commercial operator who understood what kind of company this technology would actually need to be.
Carlos Bhola arrived in the Pittsburgh microneedle orbit in 2022. Bhola’s background was atypical for the space. He had trained in engineering at Carnegie Mellon in the 1980s, spent the early part of his career at Boston Consulting Group and Credit Suisse First Boston, and then moved through a series of operating roles that traced the arc of the early consumer internet and the rise of mobile: Eachnet, the Chinese marketplace acquired by eBay; Vonage, the voice-over-IP pioneer; Here, the digital mapping division Nokia spun out; and Celsius Capital, the technology investment firm where he served as Managing Director. He had seen, up close, how a technology platform becomes a consumer product, and how consumer revenue can build infrastructure that direct scientific investment cannot. He looked at the microneedle field and saw what nearly thirty years of investors, for understandable reasons, had failed to see. Every serious attempt at commercialization had started at the top of the therapeutic pyramid, where regulatory review was longest, capital cycles were tightest, and no revenue arrived for a decade or more. The field had been trying to launch its platform off the hardest product instead of the easiest one.
Panther Life Sciences was incorporated on September 25th, 2023, and turned the historical playbook on its head.
If the microneedle patch is eventually going to transform vaccine delivery, pandemic response, oncology, and chronic disease management, as the Pittsburgh research community believes, and as Helena believes, the right place to start is at the easier end of the therapeutic pyramid: the markets where a microneedle patch is the most obviously better product available today, where the regulatory path is fastest, where the margins are highest, and where customer will pay. Those markets are cosmetics, and prior-approved dermatological therapeutics. Vaccines and novel cancer immunotherapies sit behind them, carried forward on manufacturing and regulatory infrastructure that the earlier products will have already built.
The first Panther product in the clinic is a long-lasting hyaluronic acid patch for skin aging. Hyaluronic acid is the active ingredient behind one of the largest segments of the non-invasive cosmetic market, currently delivered through injections administered in dermatology offices and medical spas. A patch version is applied at home, holds the active agent in the dermis for roughly four weeks, and requires no clinician. The first-in-human study began in 2025. Panther is targeting market entry by the end of 2026 under FDA De Novo clearance. It will be the first at-home microarray cosmetic of its kind.
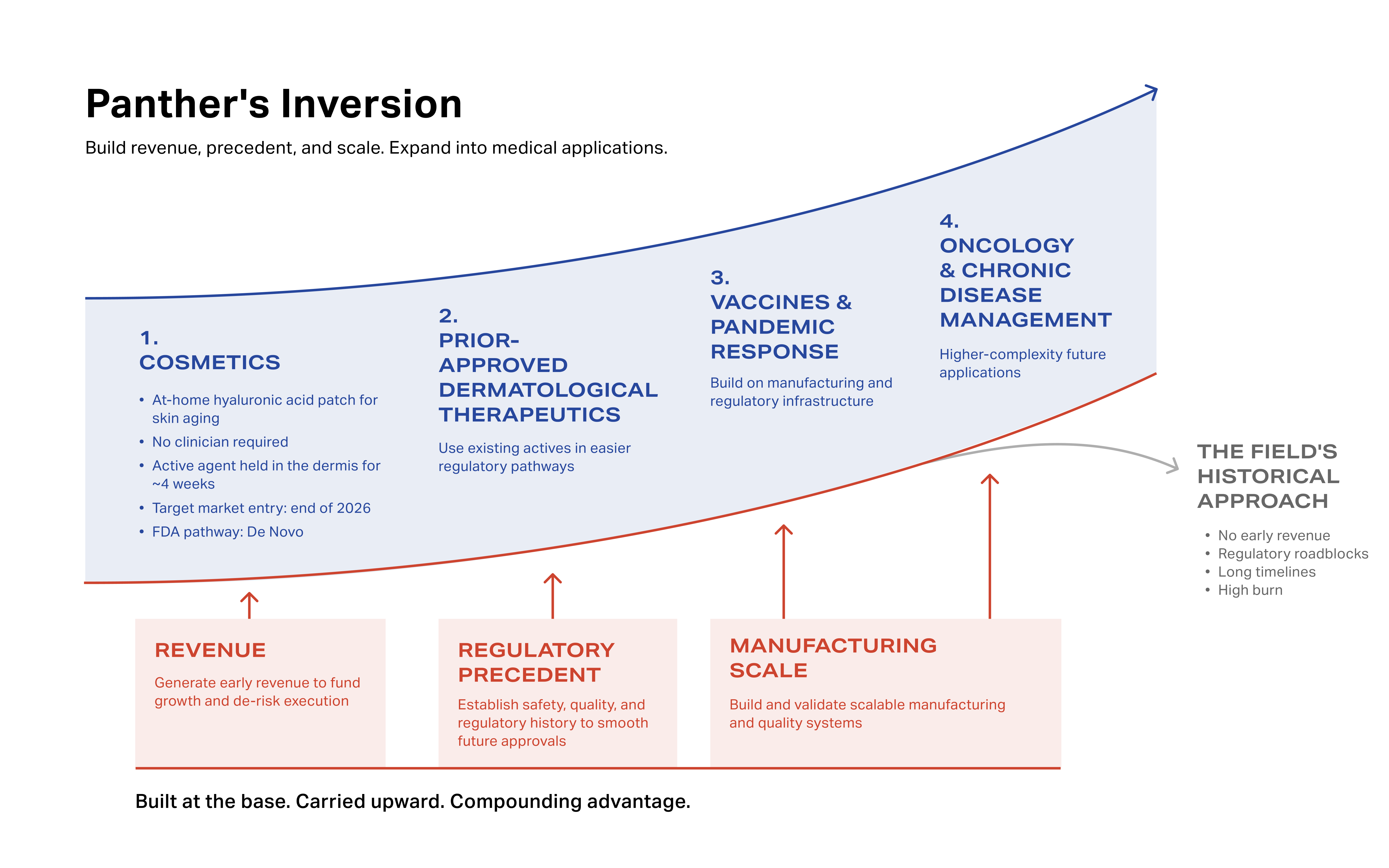
Behind it is a reformulation of an already-approved treatment for actinic keratosis. Actinic keratosis is a rough, precancerous lesion caused primarily by long-term sun exposure. It affects more than forty million Americans, with reported prevalence as high as eighteen percent in adult populations of temperate regions worldwide, and a substantial fraction of lesions, left untreated, progress to squamous cell carcinoma. The standard topical treatments, fluorouracil and imiquimod, are effective in the laboratory and under-used in practice; adherence rates are below fifty percent, driven by four weeks of burning, peeling, and flaking skin that most patients cannot tolerate.22 Panther’s reformulation delivers the same active agents directly into the correct skin layer, with less surrounding inflammation, materially better compliance, and the prospect of completion rates substantially higher than the current standard. Panther is targeting FDA approval and market entry around 2028.
Behind those near-term products sits a longer-term pipeline. The infectious disease vaccines that Panther’s research partners have been developing for years, against pandemic-class pathogens including influenza and the Nipah and Hendra viruses, sit several years out, behind the cosmetics and dermatology launches that will fund and prove the manufacturing line. Tolerance-induction work for peanut allergy and autoimmune disease sits further back still. That is the discipline.
This inversion is the point. A hyaluronic acid patch sold at a pharmacy in 2026 is, on its face, a cosmetic product. Viewed over a longer horizon, it is the beginning of the infrastructure through which a pandemic vaccine will travel to a household, delivered by mail. Every sale underwrites the manufacturing line that will, in time, produce that vaccine. Every conversation with the FDA on the cosmetic device establishes precedent for the therapeutic, and eventually for platform approval. Platform approval is the regulatory status Panther is building toward, in which the microneedle patch itself is accepted as an established route of administration, onto which appropriately reformulated drugs and antigens can be loaded with streamlined for review. This is the step the field has been missing, and no one has tried to sequence the problem this way.
The Device and the Factory
A Panther microarray patch is a small adhesive backing, roughly the size of an ordinary bandage, carrying an array of a few hundred dissolvable microneedles on its underside. Each needle is between two and three hundred microns long, long enough to penetrate the outer layers of the skin and short enough to stop before the pain-sensitive nerves. An applicator the size of a credit card delivers the patch with uniform pressure and depth. A patient presses it onto a prepared area of skin, typically the forearm. Within a few minutes, the needles dissolve, releasing their payload into the dermis.
The engineering achievement that makes the rest of the platform possible is shelf stability without a cold chain. A dose of active pharmaceutical ingredient is mixed into the tips of the patch. The polymer, once set, locks the drug molecules in, preventing decay. Patches manufactured in Pittsburgh in the spring of 2024 and stored at room temperature for a year retain the same immunogenicity they had the day they came off the line. This is the result the microneedle field has been chasing since Prausnitz’s first Georgia Tech papers, and it is the precondition for everything a commercial platform is meant to do. A patch that can sit in a mailbox in Phoenix in July, or in a cargo hold over Kinshasa, and still work when it reaches its patient is a different kind of object than a vaccine that requires a freezer.
The design of the patch itself is a study in deceptive simplicity. Because the active ingredient sits in the tips of the needles rather than throughout the array, and because intradermal delivery produces a stronger immune response per unit of antigen than intramuscular injection, the amount of active material required per patch is a fraction of what an intramuscular dose would require. For every COVID shot the world manufactured during 2021, the same antigen stockpile would have produced an order of magnitude more microarray-delivered equivalents, and those patches could have shipped in envelopes.
The rest of the platform is an integrated device-and-data system. Every patch carries a unique identifier, enabling tracking through returnable packaging with built-in shipping-condition sensors. Every applicator validates correct placement, and every application streams data into a cloud layer that connects real-world usage back to the patient’s medical record. In its current form the system is designed for clinical trials; however, in its eventual form, it is designed to be the delivery endpoint of a global pharmaceutical platform: a patch that knows who it is, where it has been, and whether it worked.
The intellectual property that sits around the system is among the most extensive in the field. Panther holds or has filed more than three hundred patents. The estate is the result of more than a decade of foundational research in Pittsburgh, and it covers most of the ground a credible commercial entrant in the category would need to occupy.
Manufacturing is the piece that has broken every previous attempt, and it is the piece Panther has spent the most time solving. The production program is anchored at Pitt BioForge, the University of Pittsburgh’s advanced biomanufacturing institute. Under an automation program now in its final stages, Panther is building a fully automated line designed to take the manufacture of microarray patches out of the artisanal range that has historically priced the field out of mass-market application, and into the unit economics that a consumer cosmetic, a dermatology therapeutic, and eventually a globally-deployed vaccine each require. Current Good Manufacturing Practice (cGMP) production for clinical supply and market entry moves through a contract development and manufacturing partner. A factory built to that scale can produce a patch for less than the cost of any intramuscular alternative in the world. A supply chain that can mail that patch can reach every household on Earth.

Pittsburgh, DARPA, and the Vaccine Community
Pittsburgh is not where most people expect a biotechnology company of this kind to come from. The city is better known, in the popular imagination, for its three rivers and for the steel industry that once anchored them. But the Pittsburgh of 2025 is a different city, and Panther is one of its defining companies.
Over the last three decades, Pittsburgh has become one of the most concentrated biomedical research ecosystems in the United States. The University of Pittsburgh Medical Center, or UPMC, is one of the largest health systems in the country, with forty hospitals and a research budget that rivals the Ivy League. Across Schenley Park, Carnegie Mellon runs the deepest robotics and machine-learning programs in the country and a top-ten engineering school. Between the two universities, the city houses one of the densest concentrations of bioengineering, precision manufacturing, and clinical research capacity to be found anywhere. The explicit goal of the current civic and institutional leadership, and of the federal programs that have invested in the city over the last five years, is to turn that concentration into industrial output. Pitt BioForge, the advanced biomanufacturing institute at the heart of the effort, was created for precisely that purpose. Panther is one of its earliest, and most ambitious, anchor tenants.
The company’s leadership reflects that anchor. Its CEO, Carlos Bhola, is a serial entrepreneur and Carnegie Mellon engineering graduate whose operating record runs from early consumer internet through mobile and consumer goods. Its manufacturing program is run out of Pitt BioForge by Ken Gabriel, whose career is one of the rare operator arcs in American science that includes both DARPA and Google. Gabriel founded and ran DARPA’s MEMS Program in the 1990s and later served as Deputy Director of the agency. He ran Advanced Technology and Projects at Google. He was the founding Chief Operating Officer of Wellcome Leap, the global health-research organization funded by the Wellcome Trust. He holds a PhD from MIT. He is one of a small number of operators in the world who has actually scaled microsystem fabrication from prototype to production, across domains, at government and industrial scale.
Around him sits a deep bench of Pittsburgh-based engineers and clinicians. Douglas Weber, a Carnegie Mellon mechanical engineer and DARPA neural-engineering veteran, runs device engineering. Brian Rogers, a veteran technology leader, runs engineering and product development. Gary Fedder, the Carnegie Mellon electrical and computer engineer who is widely regarded as one of the country’s leading experts on microelectromechanical systems, sits on the scientific team. Louis Falo, the Chair of Dermatology at the University of Pittsburgh and the researcher whose laboratory produced much of the original skin-vaccine work, remains central to the scientific program. Emrullah Korkmaz, the young Pittsburgh bioengineer whose manufacturing techniques helped make the platform possible, runs the microneedle and microarray research.

The research reach extends beyond Pittsburgh. Christopher Broder, the Chair of Microbiology, Immunology and Infectious Diseases at the Uniformed Services University of the Health Sciences, leads the infectious disease and pandemic vaccine work from Bethesda; his group has been central to U.S. biodefense vaccine research for more than two decades. Isaac Chiu at Harvard Medical School, whose work on neuroimmunology and allergic inflammation underpins the tolerance-induction work, and Niroshana Anandasabapathy at Weill Cornell, whose clinical research focuses on skin cancer and dermatologic immunology, round out the external scientific bench.
The advisory group extends the reach into adjacent fields. Geoff Ling, the founding director of DARPA’s Biological Technologies Office and a retired U.S. Army colonel, brings the defense-research perspective that shaped a generation of pandemic preparedness thinking. Anantha Shekhar, the Senior Vice Chancellor for Health Sciences at the University of Pittsburgh, anchors the institutional relationship with UPMC. Charbel Bouez, a former Senior Vice President of Global R&D at International Flavors & Fragrances, who spent fifteen years at L’Oréal leading regenerative beauty and skin research, anchors the commercial strategy for the cosmetics and dermatology launches. Anthony Sun, the CEO of Zentera Therapeutics and co-founder of Zentalis, and Bo Shao, the founding managing partner of Matrix Partners China and a co-founder of Eachnet, anchor the financial and commercial advisory bench.
A Lever on the Infrastructure of Medicine
Helena invested in Panther because Panther is working on one of the most consequential, and most under-resourced, levers in global public health: the infrastructure through which medicine reaches the human body.
In the modern era of medicine, delivery has become the bottleneck. That is the lesson of COVID-19. The vaccines themselves were one of the great scientific feats of the century. The system that was supposed to deliver them was not. It is also the lesson of MPox in 2022, of routine pediatric immunization gaps across the developing world, and of every clinical condition for which a working therapy exists but cannot reliably reach the patients who need it. We can make the medicine. We cannot, in most of the world, deliver it.
The cold chain, the syringe, the clinician, and the intramuscular dose are the four hidden assumptions on which almost every vaccine and injectable therapeutic in the world currently depends. They are the reason a COVID vaccine requires a freezer and a trained nurse. They are the reason fourteen million infants in low-income countries received no routine vaccinations last year. They are the reason the world’s pandemic response is bottlenecked on antigen supply even when the science is ready. Each of these constraints looks, on close inspection, like a choice more than a necessity. A shelf-stable microarray patch, mailed to a doorstep and self-applied, removes all four of them.
Panther also sits at the center of a thesis Helena has been working on for the better part of a decade. Through our Biosecurity project, we have spent several years in conversation with the experts who shape U.S. and international preparedness, including pandemic-response operators, scientists, federal officials, and members of the intelligence community, about what it would actually take to blunt the next biological catastrophe before it arrives. One of the clearest and most persistent conclusions of that work is that scientific capability has outrun delivery infrastructure. We now live in a world in which a pandemic vaccine can be designed and produced in a matter of weeks. We do not yet live in a world in which it can actually reach the people who need it. Panther is building, quietly and commercially, the physical layer of that second problem.

We are aware that this particular promise has been offered, in substantially similar form, many times before. The fact that the field has failed for thirty years is the most important single piece of information on which our investment thesis rests. It is precisely because the history is long, and littered with well-intentioned failures, that the strategic discipline Panther has shown matters. Panther’s cosmetics-first sequencing is the strategic recognition, made in advance, of which dollar of revenue will keep the company alive long enough to build the infrastructure that every previous company in the field has run out of money trying to assemble. That discipline is the difference between the company that lands this technology and the next in a long line of companies that will not.
We are also aware that a platform approval for the microneedle patch, should Panther obtain one, has implications that extend well past its own pipeline. The patch becomes a general-purpose delivery route into which any appropriately reformulated small molecule, peptide, or antigen can be loaded. The economics of pandemic preparedness change. The economics of global vaccine equity change. The economics of oncology immunotherapy and the daily management of chronic disease begin to change. The set of people who have practical access to therapies that currently require a clinician, a cold chain, or an expensive intramuscular dose widens considerably.
Helena’s role with Panther, consistent with how we work across the our firm, is not only capital. It is the strategic and commercial relationships that speed the company’s arrival at its flagship-customer inflection. The Helena network includes many of the public-health leaders, pandemic-response operators, employers, insurers, and retailers likeliest to be among the earliest consequential buyers of a commercial microarray platform. Panther is in the Goldilocks Zone we look for: transformative technology that works, a commercial path in view, a team capable of holding the plan, and a moment just ahead of broad recognition that the technology is finally ready.
A Different Route into the Body
If Panther succeeds, the future looks different.

A parent in rural Nigeria opens an envelope delivered by the national postal service that morning. Inside is a sheet of four shelf-stable patches, labeled for each member of the household. The child’s flu vaccine, the grandfather’s pneumococcal booster, and the family’s annual MMR. There is no clinic to walk to, and no needle to fear. The patches are applied at the kitchen table, in a few minutes, by the patients themselves.
A school nurse in rural Arkansas, in the middle of a bad influenza season, receives a weekly shipment of pediatric patches that she distributes to homeroom teachers. Vaccination rates in her district, stuck for a decade at under forty percent, pass seventy.
A public health commissioner in a small Central American country, four weeks into an outbreak of a respiratory pathogen she has never seen before, orders a hundred thousand doses of a newly-formulated patch from the country that manufactured them. They arrive in cardboard boxes a week later. She distributes them through the national postal system, and the outbreak stalls before it reaches the capital.
A retired construction worker in Phoenix, who has spent thirty years working under the desert sun and has had four pre-cancerous lesions removed from his face by a dermatologist, applies a course of patches at home over four weeks. The standard topical creams he gave up on the year before, after seven days of burning and peeling that he could not tolerate, have been replaced by a treatment he can complete on his own. The lesions resolve, and none becomes cancer.
A child with a peanut allergy is desensitized at home, over a period of eighteen months, by a monthly patch that her parents pick up at the pharmacy. She outgrows the allergy the way children once outgrew other allergies more often than they do now, slowly, gradually, safely. She eats a peanut butter sandwich on her twelfth birthday.

Each of these futures hinges on a single change: delivering medicine into the skin, rather than through it.
That change has been on the list of civilizational upgrades humanity has been moving toward for centuries. Chinese practitioners were already inoculating against smallpox through nasal insufflation by the sixteenth century. Lady Mary Wortley Montagu sketched the practice anew in Constantinople in 1717. Onesimus and Zabdiel Boylston demonstrated it in Boston in 1721. Edward Jenner formalized it into vaccination in Gloucestershire in 1796. Benjamin Rubin’s bifurcated needle helped scale it into a global public-health campaign in 1961. The World Health Organization used it to eradicate smallpox in 1980, the first human disease eliminated from the wild. Mark Prausnitz’s laboratory reintroduced its modern plausibility in 1998. The Food and Drug Administration made it federal policy in an emergency in 2022.
Panther, in Pittsburgh, is building the last and most important piece. The patch will be manufacturable, shelf-stable, commercially durable, and capable of carrying whatever payload the world needs it to carry, to wherever in the world it needs to go.
We are proud to be early investors. We are looking forward to what the next decade of this work will make possible.
Variolation is an 18th century smallpox immunization technique in which a small amount of material from a smallpox lesion was introduced into a small skin wound, producing a controlled, generally milder infection that conferred lifelong immunity. Practiced in China, India, and parts of Africa for centuries before being introduced to Europe in the early 18th century.
The continuous temperature-controlled supply chain required to keep a temperature-sensitive medical product stable from manufacturer to patient. Most modern vaccines require unbroken refrigeration; some, such as the original Pfizer COVID-19 vaccine, require ultra-cold storage at -60°C to -80°C.
Intradermal injection delivers a drug into the dermis, the immune-rich middle layer of the skin. Intramuscular injection delivers it into a deeper muscle layer. Most modern vaccines use intramuscular routes for ease of administration; intradermal routes are increasingly recognized as more efficient for many immune-active payloads.
Langerhans cells are antigen-presenting immune sentinels that sit in the epidermis, named for Paul Langerhans, who described them in 1868.
Dendritic cells are a broader family of antigen-presenting immune cells found throughout the body, characterized by Ralph Steinman at Rockefeller University in 1973. Together they make the skin the body’s most immunologically active accessible tissue.
The outermost layer of the epidermis, composed of dead, keratin-rich cells. Acts as the body’s primary barrier against external chemicals, pathogens, and water loss. Difficult for most molecules to penetrate, which is why microneedles must mechanically pierce it.
An FDA category for products that combine two or more regulated components, typically a drug and a device. Combination products are reviewed under both regulatory pathways, which can substantially extend approval timelines and capital requirements.
A regulatory pathway by which the FDA classifies a novel medical device with no existing predicate. Once cleared, it establishes the regulatory framework for future similar devices to follow the simpler 510(k) pathway.
A rough, scaly precancerous skin lesion caused primarily by long-term ultraviolet exposure. Common in adults over forty in temperate climates. Untreated lesions can progress to squamous cell carcinoma, a form of skin cancer that, while generally treatable when caught early, accounts for tens of thousands of deaths annually.
Current Good Manufacturing Practice. The FDA’s quality and process standards required for the production of pharmaceutical and biological products. cGMP compliance is a precondition for clinical supply and market entry.
Shelf stable refers to products that can be safely stored at room temperature for extended periods without degrading or losing effectiveness. In medicine, this eliminates the need for constant refrigeration, significantly streamlining distribution logistics.
Helena’s purpose is to identify solutions to global problems and implement them through projects. Each project is a separate, unique effort.
Sometimes, we believe that the most effective method to implement a project is through for-profit action, including investment and/or the founding and operation of businesses.
These projects are designated as “profit” on their associated project pages on this website. This page is an example of such a project.
To implement efforts through for-profit means, entities(s) including Helena Special Investments, LLC, a privately-owned limited liability company that operates in business activities that have the potential to transformatively address societal problems while targeting attractive returns to investors, are utilized.