
Seeing the Signal Before the Storm
Editor’s Note: This paper builds on discussions at Helena’s Mexico Summit and ongoing conversations within our community about AI, biological risk, and governance. It reflects a growing recognition that preventing catastrophic biological harm will depend not only on norms and safeguards, but on our collective ability to detect and interpret early signals across fragmented systems — before crises escalate.
Over the past two decades, we have grown accustomed to describing pandemics and biological emergencies as “once-in-a-generation” events. That framing no longer holds. What we are facing is not a sequence of rare shocks, but a structural shift in risk—one driven by climate disruption, ecological pressure, global mobility, and the accelerating convergence of artificial intelligence with the life sciences.
Recent debates about AI and biosecurity often frame the challenge as a stark choice: either a tightly controlled surveillance state, or a future of chaotic misuse enabled by rapidly diffusing technologies. This is a false binary. The real vulnerability lies elsewhere—in our inability to see emerging biological threats early enough to act with restraint, proportionality, and confidence.

At the Helena Summit in Mexico, a recurring theme surfaced across otherwise diverse conversations: our capacity to respond to biological crises now outpaces our ability to anticipate them. We have become better at mobilizing countermeasures once a threat is recognized. Yet we remain dangerously weak at detecting early signals, connecting fragmented data across borders and sectors, and equipping policymakers with usable intelligence before crises escalate.
This gap is not primarily a failure of science or goodwill. It is a failure of system design.
The question before us, then, is not simply how to prepare better for the next pandemic, but how to design an integrated biosurveillance apparatus that can detect emerging biological threats early, translate weak signals into actionable insight, and do so in a way that is ethically governed and politically usable.

The Limits of Today’s Defenses
Despite unprecedented investment since COVID-19, the global biosurveillance landscape remains siloed and fragmented. Clinical surveillance detects outbreaks only once illness is widespread. Genomic surveillance has expanded rapidly, but remains uneven, pathogen-specific, and poorly integrated with other data streams. Environmental monitoring—of wastewater, air, or water—is increasingly feasible but rarely linked systematically to clinical or epidemiological intelligence. Data systems remain siloed by discipline, institution, and jurisdiction.
These shortcomings reflect surveillance systems designed for a slower, more linear world—one in which outbreaks were expected to be local, attribution relatively straightforward, and response windows measured in weeks rather than days.
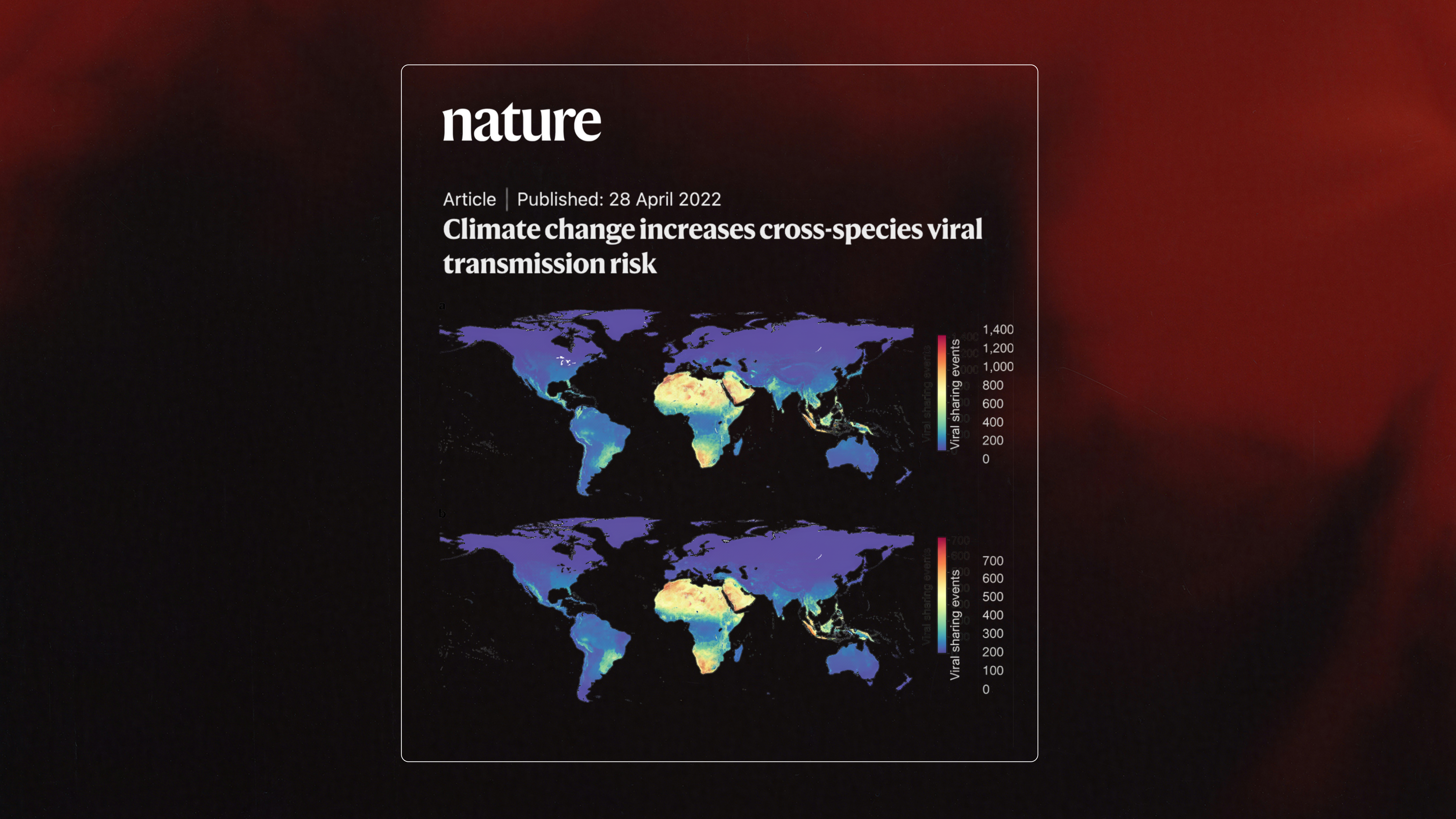
That world has changed. Zoonotic spillover is accelerating as climate change reshapes ecosystems and increases contact between wildlife, livestock, and humans. Global mobility compresses detection windows, allowing pathogens to cross continents before alarms are raised. At the same time, advances in synthetic biology and AI-enabled protein design are lowering barriers to engineering biological systems in ways that challenge long-standing assumptions about origin, intent, and attribution. Analyses in Nature and Nature Climate Change suggest that emerging infectious disease events are increasing in frequency and diversity, driven by precisely these anthropogenic pressures.
In this context, surveillance that relies primarily on confirmed diagnoses is surveillance that arrives too late.
From Monitoring Disease to Biological Intelligence
Required now is a shift from disease-specific monitoring toward biological intelligence: the ability to detect, interpret, and contextualize weak signals across multiple domains before they converge into crisis, a bio-shield in a manner of speaking.
An effective biosurveillance system for the current era must integrate at least five streams: clinical anomaly detection; community sentinel surveillance; environmental monitoring at points of aggregation such as cities and transport hubs; One Health and veterinary surveillance at human–animal interfaces; and carefully governed contextual data, including mobility patterns.
Crucially, these streams must not merely coexist. They must be analytically fused, with pre-defined escalation pathways that determine when a weak signal becomes actionable intelligence. This is the distinction between collecting more data and building surveillance that genuinely informs decisions.
The design logic behind a bio-shield—a biosurveillance architecture developed in response to these gaps—is that early warning emerges not from any single technology, but from the integration of multiple imperfect signals into a coherent system of intelligence.

How an Integrated System Works
We do conceive of a bio-shield as an entity with a global command centre or having a monolithic platform. It is a distributed architecture designed to work with, rather than replace, existing institutions. Its core innovation lies in how it structures escalation.
At baseline, systems rely on routine diagnostics and targeted sequencing, which provide speed and scale. When anomalies appear — unusual clinical clusters, unexpected genetic signatures, unexplained severity — analysis escalates to metagenomic sequencing, capable of detecting novel or unexpected biological material without prior assumptions. In rare but high-consequence cases, deeper investigation is triggered, including engineered-feature analysis to assess whether observed patterns are consistent with natural evolution or suggest artificial modification.

This tiered approach is both operationally feasible and politically stabilizing. Resources are concentrated only when risk justifies depth, and not every signal trigger maximal scrutiny. The result is a system that reduces both false reassurance and unnecessary escalation.
The technical components already exist. Aircraft wastewater surveillance has detected viral lineages before clinical systems. Traveller-based genomic surveillance has identified variants of concern weeks ahead of domestic reporting. Distributed genomic networks—from South Africa to India to the UK—have demonstrated that high-resolution sequencing can operate at scale. The challenge is not feasibility; it is integration.


Governance by Design, Not Afterthought
The convergence of AI and biosurveillance raises a deeper question—one that sits at the heart of Helena’s work: how to build systems that protect without becoming surveillance states, and that deter misuse without amplifying it.
Advanced analytics make early detection possible, but they also raise legitimate concerns about misattribution, over-reaction, and loss of trust. Tools that assess engineered features are essential in an era of AI-enabled biology, yet they must be governed carefully to avoid misuse or geopolitical misinterpretation.
The answer is not to avoid these tools, but to constrain them with ethically-informed guardrails—through proportionality, transparency, and human-in-the-loop decision-making. BioShield’s design embeds governance at every stage: tiered data-sharing models that preserve sovereignty, dual-use risk gates that control access to sensitive analyses, and benefit-sharing mechanisms that ensure contributors are partners rather than sources.
Surveillance should inform policy, not automate it. The goal is not prediction with certainty, but decision advantage under uncertainty.
Why Geography and Equity Matter
One of the least acknowledged realities of global health security is that many of the earliest signals of future global threats emerge in regions with the least analytic capacity to act on them (which is why defunding the developing world is shortsighted). Africa sits at the intersection of high biodiversity, rapid urbanization, climate vulnerability, and expanding scientific capability.
Over the past decade, African institutions have demonstrated global leadership in genomic surveillance, often detecting variants of concern earlier than wealthier regions. Yet environmental and multisectoral surveillance remain under-resourced, and analytic integration is limited.
A distributed biosurveillance network anchored in Africa—coordinated, for example, from South Africa but spanning multiple ecological and epidemiological contexts—offers not only technical advantage, but strategic wisdom. It strengthens global protection by improving visibility where emergence is most likely, while reinforcing scientific sovereignty and equity.
The Role of Philanthropy in System Design
Why has such an integrated biosurveillance system not already been built? The answer lies less in technology than in incentives. Multilateral institutions move cautiously. Governments invest primarily in response, not anticipation. Markets undervalue prevention because its success is invisible.

This creates a design gap—one that philanthropy is uniquely positioned to fill. Philanthropic actors can invest in infrastructure that precedes consensus, demonstrate feasibility, and de-risk models that others can later adopt. An 18-month pilot can show that integrated detection works. A three-year distributed network can demonstrate scalability. A five-year platform can establish sustainability.
The costs are modest compared to the trillions lost to pandemics. The returns are largely invisible—until the moment they are needed.
Acting before the storm
The lesson of recent decades is not that we lack expertise or goodwill. It is that we consistently wait for clarity that arrives only after options have narrowed. By the time signals are obvious, trust is eroded, choices are constrained, and costs multiply.
Designing an integrated biosurveillance apparatus is therefore not a technical luxury. It is a strategic necessity for an age in which biological risk is shaped as much by human systems as by microbes.
If Helena’s convening power can help shift the conversation—from response to visibility, from fragmented monitoring to biological intelligence, and from abstract risk to actionable design—it will have contributed something enduring: the capacity to see the storm before it breaks.
About the authors:
Saheer Gharbia is Professor of Pathogen Genomics and Chief Scientific Officer of Genomics Surveillance, The Wellcome Sanger Institute, Wellcome Genome Campus, Cambridgeshire, UK.
Lalitha Sundaram is Assistant Research Professor at the Centre for Pandemic Risk Management at the University of Cambridge, UK.
Wilmot James is Professor and Senior Advisor to the Pandemic Center in the School of Public Health, Brown University, Rhode Island, USA.